Vitamin D and Cognition: What the Evidence Actually Says
Roon Team
Vitamin D and Cognition: What the Evidence Actually Says
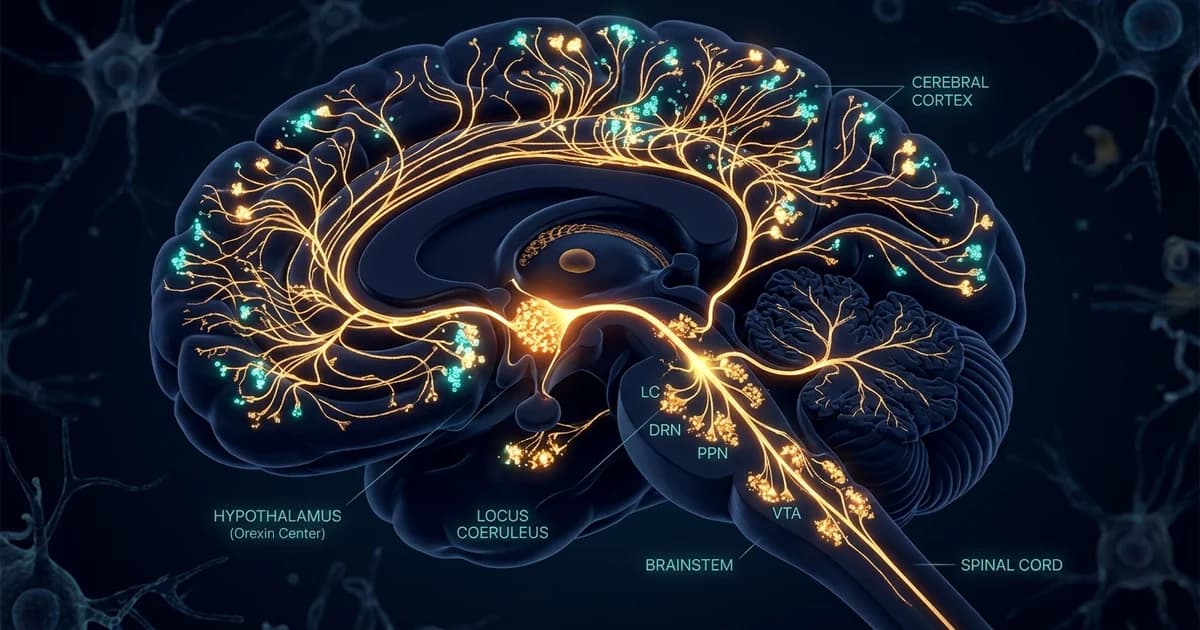
Your brain is studded with receptors for vitamin D. They sit in the hippocampus, the region that runs memory and learning, which is a strange place to find a nutrient most people associate with strong bones. That detail is the starting point for understanding vitamin d and cognition, and it explains why the question keeps showing up in serious neuroscience journals rather than just wellness blogs.
The honest answer is more useful than the hype. Vitamin D looks like a foundation for long-term brain health, not a switch you flip for a sharper afternoon. Those are two very different things, and most articles blur them.
Here is what the data actually supports, what it does not, and how to read the numbers without fooling yourself.
Key Takeaways
- Low vitamin D is linked to higher dementia risk across large population studies, but the per-person effect is small.
- Vitamin D receptors exist in the hippocampus, giving the brain link real biological grounding.
- Correcting a deficiency takes months and works on long-term risk, not on today's focus.
- Supplement trials in already-sufficient older adults mostly show no cognitive benefit.
- Think of vitamin D as a baseline you protect, not a fast-acting cognitive aid.
Why the Brain Cares About Vitamin D
Vitamin D acts more like a hormone than a vitamin, and the brain treats it that way. Researchers have documented functional vitamin D receptors in the hippocampus, the brain's memory hub, which means the active form of the nutrient can directly influence how those neurons behave.
This is the core of the vitamin d brain story. The receptors are not decorative. When the active hormone binds them, it helps regulate genes tied to neuron survival, inflammation control, and the handling of damaged proteins.
One mechanism gets the most attention in Alzheimer's research. Some work suggests vitamin D supports the clearance of amyloid beta, the sticky protein that builds up in the Alzheimer's brain. As one overview of the dementia link notes, certain studies point to vitamin D aiding the removal of these aggregates, though the findings are not uniform.
So the biology is plausible. The harder question is whether that plausibility shows up in real people, measured over real years.
Vitamin D and Cognition: What the Population Data Shows
People with the lowest vitamin D levels carry a measurably higher dementia risk than people with the highest levels. That is the cleanest statement the population data supports, and it comes from large pooled analyses rather than single studies.
A 2025 dose-response meta-analysis of 22 studies covering more than 53,000 participants found that those in the lowest vitamin D category had a 49% higher risk of dementia than those in the highest category. The relationship was linear, with each 10 nmol/L rise in vitamin D tied to roughly 1.2% lower dementia risk.
That second number matters as much as the first. The authors were direct about it: the per-person effect is small, even though the public-health impact could be larger in populations where deficiency is widespread.
A separate 2024 meta-analysis of 23 prospective studies reached a similar place. It reported that vitamin D deficiency carried about 1.42 times the risk of dementia and a 1.57-fold higher risk of Alzheimer's disease specifically.
Why Correlation Is Not the Whole Picture
These are observational findings, and observational data has a built-in trap. People with low vitamin D tend to be less active, spend less time outdoors, and have more chronic illness. Any of those could drive both the low vitamin D and the cognitive decline.
There is also reverse causality to consider. Early, undiagnosed brain decline can change behavior, keeping people indoors and away from the sunlight that produces vitamin D. The low level might be a symptom rather than a cause.
This is why the vitamin d dementia risk conversation needs trial data, not just correlation. And the trials complicate the story.
What Happens When You Actually Supplement
Giving vitamin D to older adults who are already sufficient does not reliably slow cognitive decline. That is the uncomfortable result from the best-controlled evidence, and it is worth sitting with.
The largest example is the VITAL trial, which tested 2,000 IU of vitamin D3 per day against placebo in healthy adults aged 60 and up. Across more than 3,400 participants assessed over roughly three years, supplementation did not slow cognitive decline compared with placebo.
The researchers did find one signal worth noting. There were modest cognitive benefits among older Black participants, a group with lower baseline vitamin D on average, though the authors said those results need confirmation.
That subgroup hint points to the real pattern. Vitamin D seems to help the people who are short on it, and to do little for the people who already have enough.
The Supplement Study That Looked More Promising
Not all the supplement data is flat. A 2023 prospective study published in Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring followed 12,388 dementia-free adults and found that vitamin D exposure was associated with 40% lower dementia incidence compared with no exposure.
The benefit was not uniform. As the University of Calgary and Exeter team reported, the effect was stronger in women, in people with normal cognition at baseline, and in those who did not carry the APOE e4 risk gene.
Read the two findings together and a clear shape appears. Randomized supplementation in sufficient people shows little, while population-scale supplementation, often in people who needed it, tracks with real risk reduction. The likeliest explanation is that vitamin D fixes a deficit rather than adding a bonus.
How Common Is Low Vitamin D, Really
Vitamin D insufficiency is common enough that it is worth checking rather than assuming. Estimates vary by the threshold used, but a large share of adults in northern climates fall below recommended levels, especially in winter, and rates run higher among people with darker skin and older adults whose skin makes less vitamin D from sunlight.
That prevalence is the reason the population numbers look impressive even when individual effects are small. When a deficiency is widespread, correcting it across millions of people produces a visible signal, even if any one person gains only a little.
The practical move is simple. A blood test for 25-hydroxyvitamin D tells you where you stand, and that single number is far more useful than any guess about how much sun you got this month.
Vitamin D, Memory, and the Limits of the Evidence
The link between vitamin D and memory is real but slow, and it works at the level of long-term brain protection rather than next-hour recall. This is the cleanest way to think about vitamin d memory claims.
When the hippocampus, packed with vitamin D receptors, runs short of the nutrient for years, the conditions for decline may quietly build. Correcting that over months supports the system. It does not deliver a noticeable lift to your vitamin d cognitive function during a single study session or a demanding workday.
That distinction is where most marketing goes wrong. A nutrient that protects a structure over a decade is not the same as a compound that changes how you feel and perform in ten minutes. Both can be worth having. They simply do different jobs.
How Vitamin D Compares to Acute Cognitive Inputs
Different brain inputs work on completely different timelines. Lumping a foundational nutrient together with a fast-acting one is how people end up disappointed by both. Here is a clearer breakdown.
| Input | Timeline to Effect | What It Actually Does | Best Use |
|---|---|---|---|
| Vitamin D | Weeks to months | Corrects a deficiency tied to long-term brain health and lower dementia risk | A baseline you maintain |
| Sleep | Nightly, cumulative | Consolidates memory, clears metabolic waste | The non-negotiable foundation |
| Caffeine | 30–45 minutes | Blocks adenosine, raises alertness | Acute focus, with a crash risk |
| Caffeine + L-theanine | 30–60 minutes | Alertness with less jitter than caffeine alone | Smoother acute focus |
| Roon (sublingual pouch) | 5–10 minutes | 80mg caffeine, 60mg L-theanine, 25mg Dynamine, 5mg TeaCrine for 6–8 hours of focus, no crash | A single work session or deadline |
The table makes the point better than an argument can. Vitamin D and a sublingual focus pouch are not competitors. One sets the floor over months. The other handles the next few hours.
Conclusion
Vitamin D earns its place in any serious conversation about long-term brain health. The receptors in your hippocampus are real, the dementia-risk associations are consistent across tens of thousands of people, and correcting a true deficiency is a sensible, low-cost thing to do.
Keep the expectations honest, though. The per-person effect is modest, the strongest benefits show up in people who were actually short on it, and supplementing past sufficiency does little. Vitamin D is a foundation you build and protect over months and years.
What it will never be is a way to feel sharper this afternoon. That job belongs to a different category of inputs entirely, and confusing the two leaves you let down by both.
Frequently Asked Questions
Does vitamin D improve memory?
Vitamin D supports memory indirectly and over the long term, not in the moment. The hippocampus, your memory center, carries vitamin D receptors, and chronic deficiency is linked to higher rates of cognitive decline. Correcting a low level over months helps protect that system. It does not sharpen recall during a single study session or workday, so treat it as long-term maintenance rather than an acute memory aid.
Can vitamin D prevent dementia?
The evidence suggests vitamin D is associated with lower dementia risk, but it does not prove prevention. A 2025 meta-analysis found people with the lowest levels had a 49% higher dementia risk than those with the highest, and a 2023 cohort study linked supplementation to 40% lower dementia incidence. These are associations. Randomized trials in already-sufficient adults have mostly shown no benefit, which points to correcting deficiency rather than adding extra.
How much vitamin D should I take for brain health?
There is no single dose proven to protect cognition, and more is not automatically better. The VITAL trial used 2,000 IU per day and found no overall cognitive benefit in sufficient older adults. The smarter approach is to test your 25-hydroxyvitamin D level first, then correct an actual shortfall under guidance. Megadosing carries its own risks and offers no extra cognitive payoff once you are in a healthy range.
Why does the brain have vitamin D receptors?
The brain has vitamin D receptors because the active form acts like a hormone that regulates neuron survival, inflammation, and protein handling. Researchers have confirmed functional receptors in the hippocampus, the memory and learning hub. Through these receptors, vitamin D may influence the clearance of amyloid beta, the protein that accumulates in Alzheimer's disease. This biology is why the cognitive link is taken seriously, even though human outcomes are more mixed.
Will taking vitamin D make me feel more focused today?
No. Vitamin D works on a timeline of weeks to months and targets long-term brain health, not acute alertness. You will not notice a focus boost from a dose the way you would from caffeine. If you want same-session focus, that comes from fast-acting inputs like caffeine paired with L-theanine, not from a foundational nutrient that corrects a deficiency slowly over time.
How common is vitamin D deficiency?
Low vitamin D is common, especially in northern climates, during winter, and among older adults and people with darker skin, who produce less from sunlight. This is partly why population studies show such consistent associations: when a deficiency is widespread, correcting it across many people creates a measurable signal even when each individual gains only a little. A simple blood test tells you whether you are actually low.
Foundation vs Ceiling: Where Vitamin D Ends and Acute Focus Begins
If you read this far, you already see the split. Vitamin D is a floor you raise over months. It quietly supports the brain's long-term health, and it deserves a place in your routine if a blood test says you are low. What it cannot do is change how the next two hours feel.
That is the gap Roon is built for. Roon is a sublingual cognitive pouch with 80mg caffeine, 60mg L-theanine, 25mg methylliberine (Dynamine), and 5mg theacrine (TeaCrine), designed to reach you in 5 to 10 minutes and hold 6 to 8 hours of focus with no jitters, no crash, and no tolerance buildup. It is the acute layer, not the foundation.
To be clear about what it is not: Roon is not a replacement for correcting a real vitamin D deficiency, for sleep, or for a sensible diet. Those set your baseline. If your foundation is in place and you want clean focus for a specific work session, that is the moment to try Roon.
Written by Roon Team