Why Racetams Have Such Poor Oral Bioavailability
Roon Team
Why Racetams Have Such Poor Oral Bioavailability (and Why Delivery Matters)
Swallow a 750 mg aniracetam capsule and your brain sees almost none of it. Human pharmacokinetic data puts aniracetam's absolute systemic bioavailability at roughly 0.2%, which means about 99.8% of the dose never reaches circulation intact. That single number explains most of the confusion around racetam dosing, and it sits at the center of any honest conversation about racetam bioavailability.
The molecule isn't weak. The delivery is broken.
Here is what actually happens between your stomach and your bloodstream, why some racetams survive the trip while others get demolished, and why the route a compound takes matters as much as the compound itself.
Key Takeaways
- Aniracetam's absolute oral bioavailability is around 0.2%, because it gets almost completely metabolized on first pass through the gut and liver.
- Piracetam, by contrast, is absorbed nearly completely, with oral bioavailability close to 100%.
- The difference comes down to chemistry: lipophilic, ester-containing racetams are easy targets for first-pass metabolism, while water-soluble ones pass through untouched.
- Aniracetam isn't useless at 0.2%. Most of its activity comes from an active metabolite, N-anisoyl-GABA.
- Sublingual absorption bypasses the gut and liver entirely, which is why delivery route is part of the pharmacology, not a footnote.
What Bioavailability Actually Measures
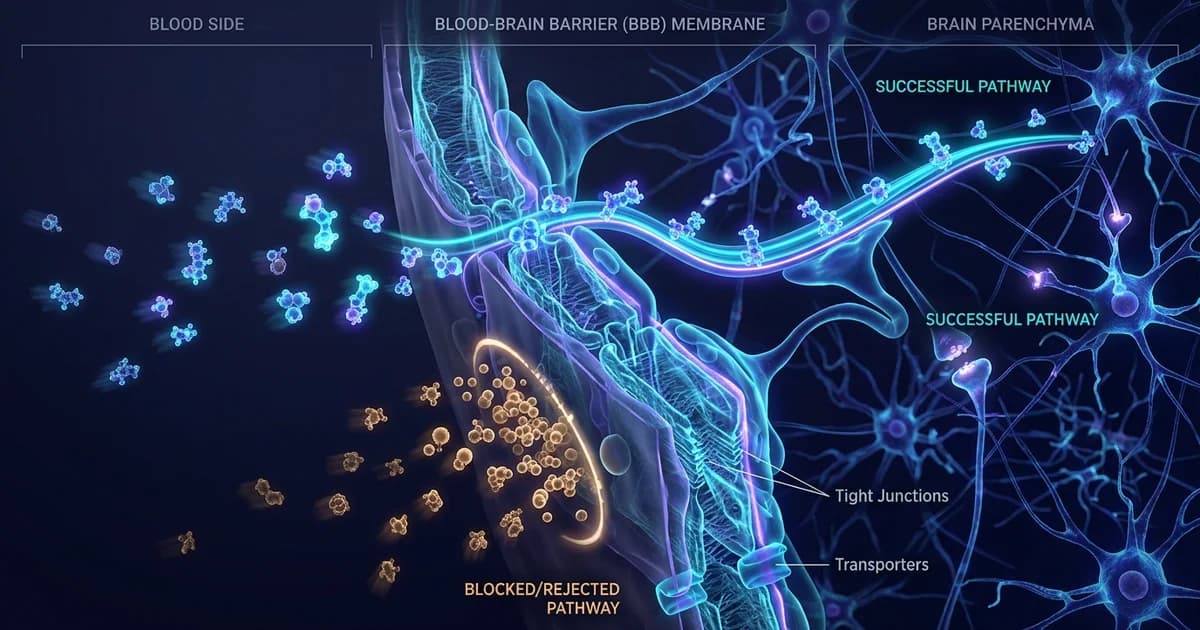
Bioavailability is the fraction of a dose that reaches your bloodstream in active form. Swallow something and it has to survive stomach acid, cross the intestinal wall, and pass through the liver before it ever circulates to your brain.
That liver pass is the problem. Blood leaving the gut routes straight to the liver through the portal vein, and the liver is built to break down foreign molecules. This is first pass metabolism, and for some nootropics it removes nearly the entire dose before it does anything.
A drug injected intravenously has 100% bioavailability by definition. Everything taken by mouth is measured against that benchmark. When you see "absolute bioavailability of 0.2%," it means an oral dose delivers one five-hundredth of what the same dose would deliver through a vein.
The Racetam Split: Why Aniracetam and Piracetam Behave So Differently
Not all racetams share the same fate, and the contrast is stark.
Piracetam is the well-behaved one. According to its European product documentation, piracetam is rapidly and almost completely absorbed after oral dosing, with an absolute oral bioavailability close to 100%, peak plasma levels about an hour after dosing, and a plasma half-life around 5 hours. A separate pharmacokinetic study in healthy volunteers confirms the near-complete absorption. Piracetam is water-soluble and stable, so the liver has little to grab onto.
Aniracetam is the cautionary tale. Research on human aniracetam pharmacokinetics found it is very rapidly and completely absorbed from the gut, yet its absolute systemic bioavailability is only about 0.2%. It gets absorbed beautifully and then gets destroyed almost immediately.
The reason is structural. Aniracetam is a fat-soluble molecule with an ester-like bond that the liver's enzymes cleave on contact. A formulation paper in PMC notes that aniracetam's low aqueous solubility and 0.2% oral bioavailability, driven by extensive first-pass metabolism, have limited its clinical use. Lipophilic compounds are the classic victims here; as one pharmacology reference explains, more lipophilic drugs are extensively metabolized in the gut wall and liver, and that first-pass clearance can produce up to 20-fold differences in blood levels between people.
So when people talk about aniracetam bioavailability, the honest framing is this: the parent molecule barely survives oral dosing at all.
But Aniracetam Still Works. Here's the Twist.
If aniracetam only reaches 0.2% bioavailability, how does anyone feel anything?
Because the metabolites do the work. When the liver breaks aniracetam down, the dominant product is N-anisoyl-GABA, which accounts for roughly 70 to 80% of metabolites, alongside p-anisic acid and 2-pyrrolidinone. Per Wikipedia's summary of the pharmacology, these metabolites are believed to carry much of aniracetam's activity.
The plasma numbers make this concrete. A LC-MS/MS pharmacokinetic study reports that about 70% of the parent drug is biotransformed into the active metabolite N-anisoyl-GABA. Independent analysis notes that parent aniracetam plasma levels sit around 5 to 15 μg/L while N-anisoyl-GABA reaches 5 to 15 mg/L, roughly a thousand-fold higher.
This is a case where "low bioavailability" of the parent compound is genuinely misleading. You are mostly dosing a precursor. The catch is that first-pass conversion is variable between people, which is part of why aniracetam effects feel so inconsistent from one user to the next.
How the Common Racetams Stack Up
Here is the oral bioavailability picture across the racetam family, plus where a fast-onset sublingual cognitive product fits for comparison.
| Compound | Approx. oral bioavailability | Time to peak | Notable trait |
|---|---|---|---|
| Piracetam | ~100% | ~1 hr | Water-soluble, survives first pass |
| Oxiracetam | ~75% | 1–2 hr | Largely excreted unchanged in urine |
| Pramiracetam | High (lipid-soluble, fat-dependent) | ~1–3 hr | Absorption tied to fat intake |
| Aniracetam | ~0.2% (parent) | Very fast, then destroyed | Works mainly via N-anisoyl-GABA metabolite |
| Roon (caffeine + L-theanine + Dynamine + TeaCrine) | Sublingual, bypasses first pass | ~5–10 min onset | 6–8 hr focus, no jitters, no crash |
Oxiracetam lands in the middle. A pharmacokinetic study in healthy volunteers measured its absolute oral availability at 75% give or take 7%, with peak levels in 1 to 2 hours and most of the dose excreted unchanged. Pramiracetam, being highly lipid-soluble, behaves differently again, with reported half-lives in the 4 to 5 hour range and absorption that leans on dietary fat.
Roon isn't a racetam. It's in the table because it answers the delivery problem this article is about: a sublingual route that sidesteps the gut and liver entirely.
Why Delivery Route Belongs in the Pharmacology
A molecule's effect depends on how much of it reaches your brain, and the route decides that. Change the route and you can change a 0.2% problem into a non-problem.
Sublingual absorption is the clearest example. When a compound dissolves under the tongue, it crosses the thin sublingual mucosa straight into venous blood, skipping the first trip through the liver. Pharmacy references describe this plainly: sublingual delivery avoids first-pass metabolism, preventing premature breakdown of the active ingredient.
Speed follows. Buccal and sublingual caffeine, for instance, can produce effects in roughly 5 to 15 minutes versus 20 to 60 minutes for a swallowed dose, because absorption starts at the mouth rather than the gut.
This is the whole point about nootropic absorption: a compound that gets shredded on first pass through the liver can survive intact if it never goes through the gut in the first place. For the racetams, that has driven research into injectable and cyclodextrin-based formulations precisely because oral dosing wastes so much of the molecule.
What This Means If You're Choosing a Nootropic
Read the route before you read the dose. A big number on a label means little if 99% of it gets cleared before it works.
Favor compounds with established, high oral bioavailability when you swallow them, or favor delivery formats that bypass first pass when the active ingredient is fragile. Both strategies solve the same problem from opposite ends. And treat any racetam with sub-1% parent bioavailability as a metabolite play, not a direct dose, because that is what the pharmacokinetics actually show.
If you want to go deeper on the active side of the stack, our explainers on how caffeine and L-theanine work together and why onset speed matters for focus cover the other half of the equation.
The Real Lesson: Chemistry and Route Are One System
Racetams aren't interchangeable, and bioavailability is the reason. Piracetam survives oral dosing nearly intact while aniracetam's parent molecule is gone almost on arrival, with its effects carried by a metabolite the liver creates on first pass.
The takeaway isn't that low-bioavailability compounds are worthless. It's that a molecule and its delivery route are a single system, and you can't judge one without the other. A fragile compound through the wrong route is a waste. The same compound through a route that skips the gut and liver can be a different drug entirely.
Dose tells you intent. Bioavailability tells you reality.
Frequently Asked Questions
What is racetam bioavailability?
It's the fraction of an oral racetam dose that reaches your bloodstream in active form. The number varies wildly across the family. Piracetam is absorbed nearly completely at close to 100%, while aniracetam's parent molecule reaches only about 0.2%. The difference comes from chemistry: water-soluble racetams pass through the gut and liver untouched, while fat-soluble, ester-containing ones get broken down on first pass.
Why is aniracetam's bioavailability so low?
Aniracetam is lipophilic and carries a bond the liver's enzymes cleave on contact. It absorbs rapidly from the gut, then gets almost entirely metabolized before it reaches general circulation, leaving roughly 0.2% of the parent compound. Most of its activity instead comes from N-anisoyl-GABA, a metabolite the liver produces from about 70% of the dose during first pass.
Does low bioavailability mean aniracetam doesn't work?
No. Aniracetam works largely through its metabolites rather than the parent molecule. N-anisoyl-GABA, which makes up 70 to 80% of metabolites, is thought to carry much of the effect, and its plasma levels run far higher than the parent compound. The real downside is consistency, since first-pass conversion varies between people.
What is first pass metabolism?
First pass metabolism is the breakdown of a swallowed compound by the gut wall and liver before it reaches the rest of your body. Blood leaving the intestine flows directly to the liver, which metabolizes foreign molecules. For lipophilic nootropics, this can clear almost the entire dose, which is why first pass metabolism is central to understanding why some oral compounds underperform.
How does sublingual absorption change bioavailability?
Sublingual absorption lets a compound cross the thin tissue under the tongue directly into venous blood, skipping the gut and the liver's first pass. That preserves more of the active ingredient and speeds onset. For fragile, first-pass-sensitive molecules, the route can matter as much as the dose, turning a poorly absorbed oral compound into one that actually reaches circulation.
Which racetam has the best oral bioavailability?
Piracetam. Studies put its oral bioavailability close to 100%, with peak plasma levels about an hour after dosing. Oxiracetam follows at around 75%. Aniracetam sits at the bottom for parent-compound bioavailability at about 0.2%, though its metabolites do most of the work. If you're swallowing a capsule, water-soluble racetams reach your system far more reliably.
Where Delivery Solves the Problem Oral Dosing Creates
Everything above lands on one point: the route a compound takes can rescue or wreck it. Aniracetam's 0.2% problem is a first-pass problem, and the cleanest answer to first-pass loss is to avoid the gut and liver in the first place.
That's the pharmacokinetic reasoning behind Roon. It's a sublingual pouch built around the same logic that explains the racetam data: absorb through the mucosa under your tongue, skip the first trip through the liver, and reach circulation in about 5 to 10 minutes. The formula is four ingredients, 80 mg caffeine, 60 mg L-theanine, 25 mg methylliberine (Dynamine), and 5 mg theacrine (TeaCrine), tuned for 6 to 8 hours of focus with no jitters and no crash.
To be clear, Roon is not a racetam and not a substitute for one, and it won't fix aniracetam's chemistry. It's an example of the principle in action: choosing a delivery route that respects how the body actually absorbs things. If your last nootropic felt inconsistent, the route may have been the variable, not the molecule.
Written by Roon Team