Folate, Methylfolate, and the Brain: How MTHFR Shapes Mood
Roon Team
Folate, Methylfolate, and the Brain: How MTHFR Shapes Mood and Cognition
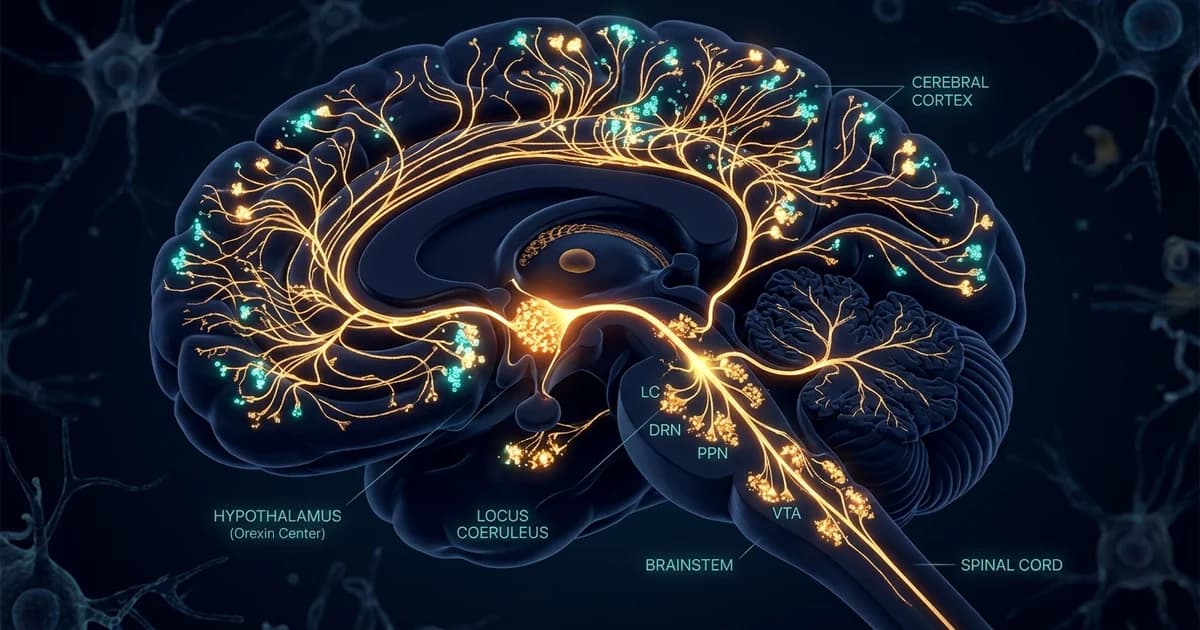
Your brain runs on methyl groups. It uses them to build serotonin, dopamine, and the myelin that insulates your neurons. The molecule that delivers most of those methyl groups is 5-methyltetrahydrofolate, the active form of folate, which is exactly why methylfolate for brain function has become one of the more interesting topics in nutritional neuroscience.
Here is the part most people miss. The folic acid in your multivitamin is not the form your brain actually uses. Your body has to convert it, and a single gene called MTHFR controls how well that conversion happens.
For a large slice of the population, that conversion runs at half speed. This article explains the biochemistry, the mood and cognition data, and why the form of folate you take matters more than the dose.
Key Takeaways
- 5-MTHF (methylfolate) is the only folate form that crosses freely into the brain. Folic acid and dietary folate must be converted first.
- The MTHFR enzyme drives that conversion. Common gene variants slow it down, lowering active folate available for brain chemistry.
- Folate feeds methylation, the process that builds serotonin, dopamine, and SAMe, the body's main methyl donor.
- L-methylfolate showed real effects in depression research when added to antidepressants, though it is not a standalone treatment.
What Folate Actually Does in the Brain
Folate is vitamin B9, and its job in the brain is to run methylation. Methylation is a simple chemical move, adding a CH3 group to another molecule, but your neurons depend on it constantly.
That single reaction sits upstream of serotonin, dopamine, and norepinephrine production. It also helps recycle homocysteine, an amino acid that becomes toxic to blood vessels and neurons when it accumulates.
The link between folate and cognition comes down to this supply chain. When active folate is plentiful, methylation runs smoothly and homocysteine stays low. When folate is scarce or stuck in an unusable form, homocysteine climbs and methyl-dependent reactions stall.
This is why folate status shows up in conversations about mood, memory, and brain aging. It is not a niche vitamin. It is a rate-limiting input for some of the most fundamental chemistry your brain performs.
The MTHFR Gene: Why the Form of Folate Matters
The MTHFR gene gives the recipe for an enzyme called methylenetetrahydrofolate reductase. Its single most important task is converting folate into its active, brain-ready form.
Methylenetetrahydrofolate reductase (MTHFR) is a key enzyme that catalyzes the conversion of N-5,10-methyltetrahydrofolate (5,10-MTHF) to N-5-methyltetrahydrofolate (5-MTHF) which is a co-substrate for the re-methylation of homocysteine to methionine. In plain terms, this enzyme is the gatekeeper between the folate you eat and the folate your brain can use.
That final product, 5-MTHF, is the workhorse. This active folate is required to recycle homocysteine into methionine, produce SAMe (the body's main methyl donor), and support healthy methylation. When methylation is impaired, systems such as energy production, hormone balance, and immune function are affected.
Here is where genetics enters the picture. Common variants in the MTHFR gene, especially the C677T variant, reduce how efficiently this enzyme works. People who carry two copies produce an enzyme that runs at a fraction of its normal capacity.
When the enzyme slows, less 5-MTHF gets made. Synthesis of 5-MTHF is the first step in methionine synthesis. Folate deficiency or a defect in MTHFR impairs the synthesis of 5-MTHF, thereby lowering the synthesis of methionine and diverting homocysteine towards the transsulfuration pathway.
This is the core of the mthfr brain conversation. A slow enzyme means you can eat plenty of folate and still come up short on the active form your neurons need.
L-Methylfolate vs Folic Acid: They Are Not Equal
The debate over l-methylfolate vs folic acid is not marketing. It is biochemistry, and the brain is where the difference shows up most clearly.
Folic acid is synthetic. Your body has to reduce it through several steps before it becomes 5-MTHF. That conversion happens mainly in the liver and depends on an enzyme called DHFR, which humans express at relatively low levels.
When you take more folic acid than your liver can process, the excess spills into your blood unconverted. This unmetabolized folic acid creates a problem at the door to your brain.
Research on the blood-cerebrospinal fluid barrier explains the mechanism. When an excess amount of folic acid is taken, it cannot be fully reduced by DHFR in the liver and unmetabolized folic acid appears in the plasma. The issue is what happens next.
Because folic acid has higher affinity to the FR1 receptor expressed at the choroid plexus than 5-MTHF, it can act as a competitive inhibitor against 5-MTHF transport from the plasma to the CSF. In addition, folic acid cannot be metabolized to 5-MTHF efficiently in the brain, which has extremely low DHFR activity. Thus, excess folic acid intake may lead to less effective folate delivery to the brain.
Read that again. Unconverted folic acid can actually block the active folate from reaching your brain. The 5-MTHF form sidesteps all of it, because it is already in the shape the brain transports and uses.
Folate Forms at a Glance
| Form | Needs MTHFR Conversion? | Brain Availability | Notes |
|---|---|---|---|
| Folic acid (synthetic) | Yes, multiple steps | Lower; excess can compete at the brain barrier | Cheap, stable, used in fortification |
| Dietary folate (leafy greens, legumes) | Yes | Moderate | Sensitive to heat and storage |
| Folinic acid | Partial | Moderate to good | Converts to 5-MTHF in gut and liver |
| L-methylfolate (5-MTHF) | No, already active | Highest; crosses the barrier directly | Bypasses MTHFR bottleneck |
The takeaway is direct. If your MTHFR enzyme is slow, the 5-mthf brain advantage is not theoretical. You are handing your neurons folate they can use without an extra step that may be broken.
Folate, Methylfolate, and Depression
The strongest clinical signal for methylfolate for brain chemistry comes from mood research, specifically depression that does not fully respond to medication.
Low folate has been associated with depression for decades. The logical question followed: would adding the active form help people whose antidepressants were only partly working?
Two trials published in the American Journal of Psychiatry in 2012 tested exactly that. They examined L-methylfolate added to SSRIs in patients who had not responded well to the medication alone.
The dose mattered. Papakostas and colleagues found that adding 7.5 mg/day of L-methylfolate was no more effective than adding placebo, but 15.0 mg/day plus ongoing SSRI treatment produced a 32% response rate, compared to 15% for augmentation with placebo. Side effects in the two groups were comparable in type and frequency.
So the higher dose roughly doubled the response rate versus placebo, with a clean side-effect profile. That is a meaningful result for a vitamin metabolite used alongside standard care.
A word of honesty here. This is folate depression research in the context of adjunctive therapy, meaning it was added to antidepressants in people with diagnosed major depression. It is not evidence that methylfolate treats depression on its own, and the brand you are reading this from makes no such claim.
What it does show is that active folate can support the methylation chemistry behind mood, particularly when that chemistry is running short.
Folate and Cognition Across the Lifespan
The connection between folate and thinking is tightly linked to homocysteine. When active folate runs low, homocysteine rises, and raised homocysteine is one of the more consistent markers tied to cognitive decline in aging.
The mechanism flows from everything above. Less active folate means less methionine, less SAMe, and a backup of homocysteine that can stress neurons and blood vessels alike.
This is why folate, vitamin B12, and vitamin B6 are studied together. They work as a unit to keep homocysteine in check, and a shortfall in any one of them can break the chain. We cover this interplay in our deeper guide to how B vitamins support brain energy and methylation and in our breakdown of homocysteine and brain health.
Across the lifespan, the practical message is consistent. Adequate active folate supports the methylation reactions that build neurotransmitters and protect neurons, while a deficiency, whether from diet or a slow MTHFR enzyme, pulls in the opposite direction.
Conclusion
Folate is not a single thing. It is a family of forms, and only one of them, 5-MTHF, slips directly into your brain to run the methylation reactions behind mood, memory, and neuron maintenance.
The MTHFR gene decides how much of that active form you can make from ordinary folate or folic acid. For people with slow variants, the form you choose genuinely changes how much usable folate reaches the brain, and unconverted folic acid can even compete with the active form at the door.
The clinical evidence is most convincing in depression, where 15 mg of L-methylfolate added to antidepressants doubled response rates in resistant cases. The broader story ties folate to homocysteine, and homocysteine to long-term cognitive health. The form, not just the dose, is what counts.
Frequently Asked Questions
What is the difference between folate, folic acid, and methylfolate?
Folate is the natural form of vitamin B9 found in food. Folic acid is the synthetic version used in supplements and fortified foods, and your body must convert it through several steps. Methylfolate, or 5-MTHF, is the active form your cells and brain use directly. The key difference is conversion: folate and folic acid both depend on enzymes like MTHFR to become 5-MTHF, while methylfolate is already in the usable shape.
Does the MTHFR gene variant really affect the brain?
The MTHFR gene encodes the enzyme that converts folate into its active 5-MTHF form. Common variants like C677T reduce that enzyme's efficiency, so carriers make less active folate from the same diet. Since 5-MTHF is the form that supports brain methylation and neurotransmitter synthesis, a slower enzyme can lower the active folate available to neurons. This does not guarantee symptoms, but it explains why some people respond better to methylfolate than to folic acid.
Is l-methylfolate better than folic acid for the brain?
For brain delivery, l-methylfolate has a clear structural advantage because it crosses the blood-brain barrier without needing conversion. Research also shows that excess unmetabolized folic acid can compete with 5-MTHF for transport into the central nervous system, and the brain itself has very low capacity to convert folic acid. For people with reduced MTHFR activity, methylfolate sidesteps the bottleneck entirely.
Can methylfolate help with depression?
In clinical research, L-methylfolate was studied as an add-on to antidepressants, not a replacement. The 2012 American Journal of Psychiatry trials found that 15 mg per day added to SSRIs roughly doubled response rates versus placebo in people who had not responded fully to medication alone. This supports methylfolate as adjunctive support for the methylation chemistry behind mood, but it is not a standalone treatment, and depression should be managed with a clinician.
How does folate affect cognition and brain aging?
Folate keeps homocysteine in check by helping recycle it into methionine. Raised homocysteine is a recognized marker associated with cognitive decline in aging, so adequate active folate supports the chemistry that protects neurons and blood vessels. Folate works alongside vitamins B12 and B6 in this process, which is why deficiencies in these B vitamins are often studied together in relation to memory and brain health.
Should everyone take methylfolate instead of folic acid?
Not necessarily. Many people convert folic acid well enough to meet their needs, and folic acid remains valuable for fortification and prenatal health. Methylfolate becomes most relevant for people with reduced MTHFR enzyme activity or those taking higher doses where unmetabolized folic acid could accumulate. The right choice depends on your genetics, diet, and goals, so it is worth discussing with a healthcare provider.
How much folate does the brain need?
There is no single brain-specific number; the adult daily reference for folate is set in micrograms of dietary folate equivalents. Therapeutic methylfolate doses used in mood research, such as 15 mg per day, are far higher than baseline nutritional needs and were studied under clinical supervision. For general health, meeting standard folate recommendations through diet and, if needed, a quality supplement is the practical target.
The Methylation Layer Behind Clear Thinking
This article is a mechanism explainer, not a product pitch, so let's be clear about where folate fits. Methylfolate is foundational nutrition. It supports the long-term chemistry that builds neurotransmitters and keeps homocysteine in range. It is not a fast-acting focus tool, and it will not sharpen your attention in the next ten minutes.
That is a different job, and it is the one Roon is built for. Roon is a zero-nicotine sublingual pouch with a focused four-ingredient formula: 80 mg caffeine, 60 mg L-theanine, 25 mg methylliberine, and 5 mg theacrine, designed for a 5 to 10 minute onset and 6 to 8 hours of steady focus without the jitters, crash, or tolerance creep.
Think of it as two layers working on different timelines. Your B-vitamin and folate status sets the foundation over weeks and months. A tool like Roon handles the acute window when you need to lock in and work. If you care enough about your brain to read 1,800 words on methylfolate, the on-demand layer is worth a look too.
Written by Roon Team